
Insomnia and obstructive sleep apnea (OSA) are the two most common sleep disorders worldwide, with each affecting about 10-30% of people1. With insomnia, a person has frequent trouble falling asleep, staying asleep, and/or waking up prematurely in the morning. These symptoms are also accompanied by daytime consequences like fatigue, difficulty concentrating, and feeling unrefreshed1.
OSA, on the other hand, is characterized by recurring episodes of narrowing or complete obstruction of the upper airway during sleep. These episodes lead to temporary decreases in oxygen levels, intensified but unsuccessful breathing attempts, and awakenings from sleep for effective breathings. Like insomnia, OSA also causes daytime fatigue and sleepiness1.
OSA and insomnia can exacerbate each other and may go hand in hand. Approximately 30-50% of patients with OSA report clinically significant insomnia symptoms and 30-40% of patients with chronic insomnia fulfil diagnostic criteria for OSA.2
Yet, this frequent co-occurrence of comorbid insomnia and sleep apnea (COMISA) remains insufficiently recognized. Its impact on individuals, healthcare systems and economies deserves more investigative focus from clinicians, policymakers, and industry leaders.
The burden of insomnia and COMISA extends far beyond disrupted sleep. Individuals living with these conditions face additional impairments in daytime functioning, and overall quality of life3. People with COMISA often experience more severe symptoms than those with either insomnia or OSA alone. They report poorer sleep quality, increased daytime fatigue, and higher rates of depression and anxiety3.
COMISA is also associated with increased risks for cardiovascular disease and recent studies have linked it to higher rates of hypertension and metabolic syndrome, especially when the insomnia is characterized by difficulty initiating sleep4. Moreover, COMISA has been associated with a 70% increased risk of all-cause mortality compared to individuals without these sleep disorders5.
Fortunately, both conditions can be treated and managed well with current guideline- recommended interventions, including digital cognitive behavioral therapy (dCBT). This reinforces the need to increase attention on patient identification and diagnosis.

Figure 1
The financial consequences of insomnia and COMISA are substantial. A landmark study from Quebec, Canada estimated the total annual cost of insomnia alone at $6.6 billion CAD, representing about 1% of the province’s GDP. These costs include direct healthcare expenses-such as consultations, medications, and hospitalizations as well as indirect costs like absenteeism and reduced work productivity6.
In the United States, the economic impact is even more staggering. A 2021 study estimates the total annual cost of insomnia in the United States to be between $150.4 billion and $174.9 billion (in 2016 USD). Narrowed down to healthcare costs alone, sleep disorders overall cost the US healthcare system $94.9 billion each year, with insomnia being the second most costly sleep disorder after obstructive sleep apnea7.
As in the Quebec study, the majority of these costs are attributed to indirect costs such as lost productivity, accidents, and errors. Given that COMISA patients tend to experience even greater health impairments, the economic burden is likely higher for this group, although further research is required to confirm this.
An analysis commissioned by the European Brain Council found that in 2010, sleep disorders (including, but not limited to, chronic insomnia) accounted for a cost of €20 billion direct and €15 billion indirect across all European Union member states, Iceland, Norway and Switzerland. In the same year, insomnia accounted for 389,753 disability adjusted life years (DALYs).8,9
Insomnia symptoms are strongly associated with reduced workplace productivity, contributing to both absenteeism (missed workdays) and presenteeism (reduced performance while at work).
In a large corporate study investigating the relationship between insomnia symptoms and workplace productivity, insomnia emerged as the strongest predictor of productivity loss— much more than even stress10.
Targeted sleep interventions, such as digital cognitive behavioral therapy (dCBT), have been shown to significantly improve employee productivity10. These findings suggest that effective treatment insomnia and COMISA benefits both employees and their organizations by improving productivity and reducing costs.
The high prevalence of insomnia and COMISA results in substantial direct and indirect costs for healthcare payers. Insomnia patients account for a disproportionately large share of healthcare spending. One US study reports that although only 9% of insured members had insomnia, they accounted for 21% of total healthcare claim spending11.
These patients use more healthcare services and often have other medical conditions that increase treatment complexity and cost. Another US study found that patients with insomnia and comorbid conditions had healthcare costs as much as 80% higher compared to those without insomnia12.
This offers a clear challenge and opportunity for payers and healthcare policy makers. Strategies to address the impact of insomnia and COMISA should include incentivizing integrated care through reimbursement policies, supporting preventive measures via public health campaigns, and funding research to identify the access barriers for the conditions. Left unaddressed, these conditions will continue to drive up healthcare utilization and associated costs.
Insomnia and COMISA are no longer peripheral concerns; they are central issues in public health. As their prevalence and substantial burden continues to rise, industry stakeholders must commit to advancing research, education, and innovative solutions to address the unmet needs of patients with insomnia and COMISA, their providers, and the broader health systems.
By prioritizing the diagnosis and effective management of insomnia and COMISA, healthcare ecosystems can achieve significant reductions in long-term economic costs and improvements in patient outcomes.
AMA
Sweetman A. Increasing burden of insomnia and COMISA. Resmed Sleep Institute. 2026. https://www.resmedsleepinstitute.com/insights/increasing-burden-of-insomnia-and-comisa
APA
Sweetman, A. (2026). Increasing burden of insomnia and COMISA. Resmed Sleep Institute. https://www.resmedsleepinstitute.com/insights/increasing-burden-of-insomnia-and-comisa
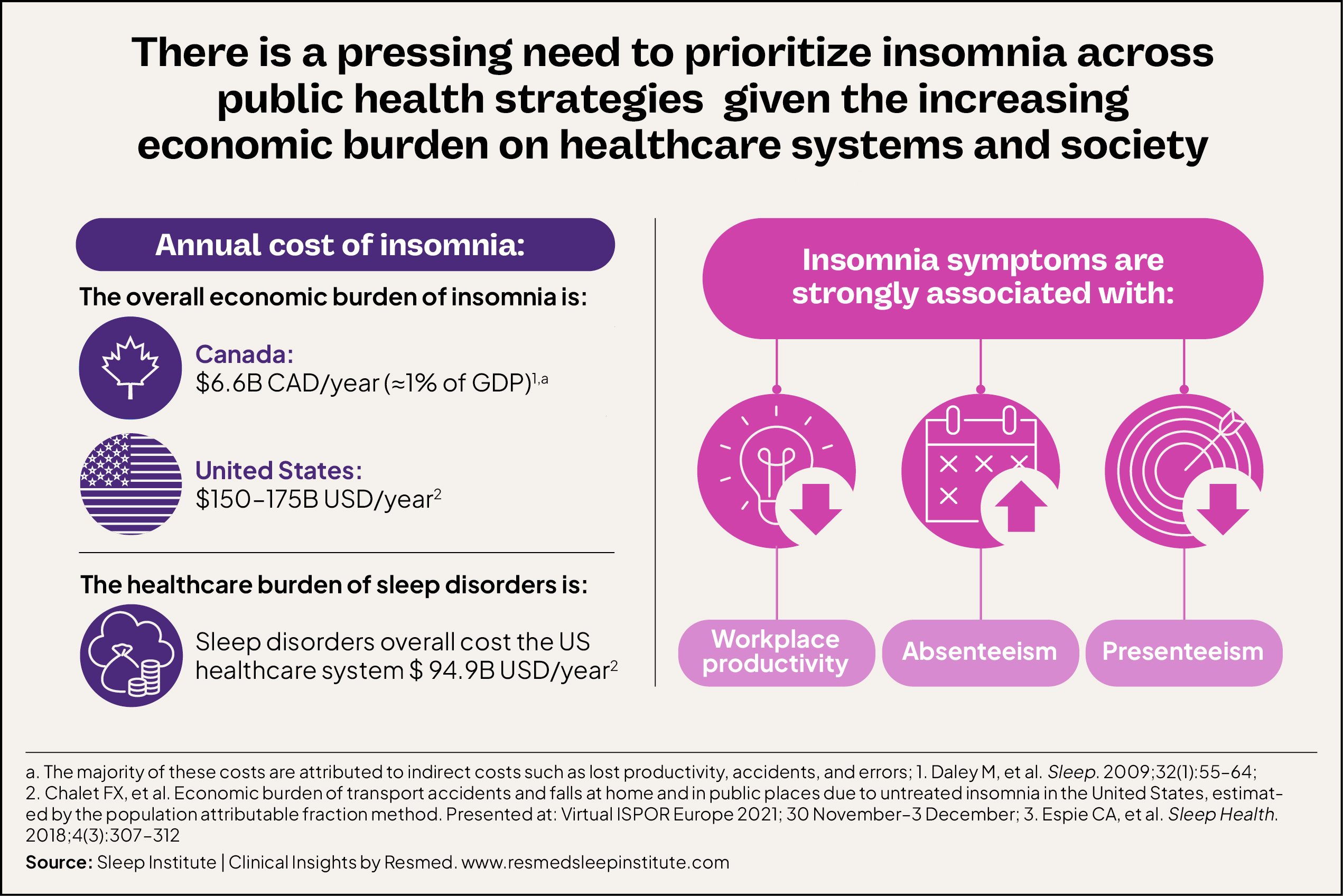 Figure 1
Figure 1